iSizing in Action: Automated EVAR Sizing & Planning with Prof. Rafaelle Spear

Endovascular aneurysm repair (EVAR) depends on the quality of pre-operative planning. A few millimetres at the proximal neck, an underestimated angulation, a missed calcification at the access vessel — any of these can turn an elective case into a complication.
Traditionally, the sizing step that underpins every device decision has been manual, time-consuming, and operator-dependent.
In this Case of the Month, Prof. Rafaelle Spear takes us through how automated sizing and interactive planning come together inside iSizing on a real abdominal aortic aneurysm case at CHU Grenoble Alpes — from CT to a fully specified endograft configuration.
Context of the Case
The patient presented with an infrarenal abdominal aortic aneurysm. Automated segmentation in iSizing immediately considered both thrombus and calcifications along the aortic wall, giving a complete picture of the anatomy before any measurement was made.
iSizing assess the proximal neck across multiple levels and provides 100 diameter measurement per slice to compute maximum and average diameter with 80000 measurements in total.
Automated Sizing Measurements
Two things jump out from this picture: a short, somewhat conical proximal neck with non-trivial angulation, and a left common iliac that widens significantly mid-vessel — both classic challenges that drive device choice and landing-zone strategy.

Why automated sizing matter?
The value of automated sizing is not just speed, though the report does land in minutes with a single click. It is consistency. Every cross-section is measured the same way. Every centreline is reconstructed identically. The surgeon spends time on judgement, not on calliper work.
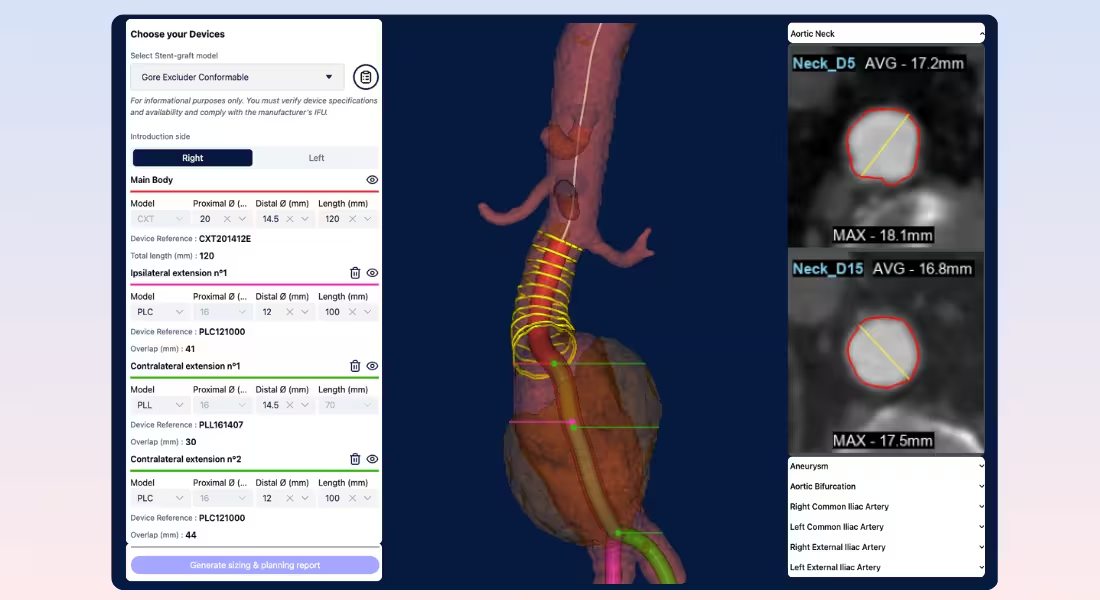
In iSizing, the workflow gives the operator two complementary views:
- An interactive 3D model that exposes the centreline, the diameters, and the calcified/thrombotic regions with a downloadable sizing report that consolidates every measurement needed for ordering and intraoperative reference.
- Cross-sectional cuts at each neck and iliac level are presented alongside the 3D view, so the surgeon can check against the raw CT before committing.
For this case, that meant Prof. Spear could see, in one glance, that the proximal neck stayed in the 16.9–17.7 mm range over the first 15 mm — confirming a usable, if short, sealing zone.
Prof. Spear's Planning Strategy
With the measurements settled, planning shifts from "what is the anatomy?" to "what fits the anatomy?"
iSizing keeps both questions on the same screen:
- The operator selects a device and immediately sees it positioned on the patient-specific 3D model, with proximal and distal baselines that can be adjusted while the device adapts in real time.
Advantages of Planning Agent
Interactive planning previews actual deployment of stent-graft in the aorta. Using iSizing, you could:
- Select devices from multiple manufacturers (Medtronic, Cook, Gore, Artivion, Terumo) inside the same workflow, without the need to remember the full device catalogue.
- Adjust the baselines and watch the endograft re-render on the 3D anatomy , so the consequences of moving a seal zone by a few millimetres were immediately visible.
- Generate the full sizing and planning report in a single click once the configuration was locked.
The result is not a faster version of the old workflow. It is a different workflow — one where device selection becomes an iterative conversation with the anatomy rather than a one-shot decision made from a stack of axial slices.
Conclusion
Three things stand out from this case:
- Automated, multi-level neck assessment is more useful providing around 100 measurements which gave Prof. Spear a clear picture before any device was selected.
- Interactive planning agent changes how planning feels. Instead of mentally projecting a device onto a CT, the surgeon sees it in place, and can swap manufacturers or adjust landing zones in seconds.
- Time saved, Sizing and planning reports that previously took an hour of manual work to build the report, It is now produced in minutes.
For complex anatomies like this one — short angulated neck, asymmetric iliacs, calcified wall — the combination of automated segmentation and interactive planning is exactly where AI-assisted tools empower vascular surgeons.