iSizing in Action: Automated EVAR Sizing & Planning with Dr. Fernando Gallardo

A Symptomatic AAA case
This case was presented with abdominal pain and local tenderness on palpation, the CT findings were: an abdominal aortic aneurysm that had grown from 4.0 cm to 4.7 cm in just three months.
Rapid aneurysm growth is one of the most significant risk factors for rupture. While the commonly cited threshold for elective AAA repair is 5.0 cm, the combination of symptoms and accelerated expansion made the decision to treat straightforward — even at 4.7 cm.
The question wasn't whether to intervene, but how to plan the intervention precisely and efficiently. This is where iSizing came in.
Automated Sizing — A Complete anatomical picture in minutes
Traditionally, EVAR sizing involves a time-consuming manual review of CT images: measuring aortic neck diameters at multiple levels, assessing iliac anatomy, calculating lengths, and documenting calcification and thrombus and sizing measurement which in itself is a burden.
It's skilled, painstaking work — and variability between operators is a known challenge.
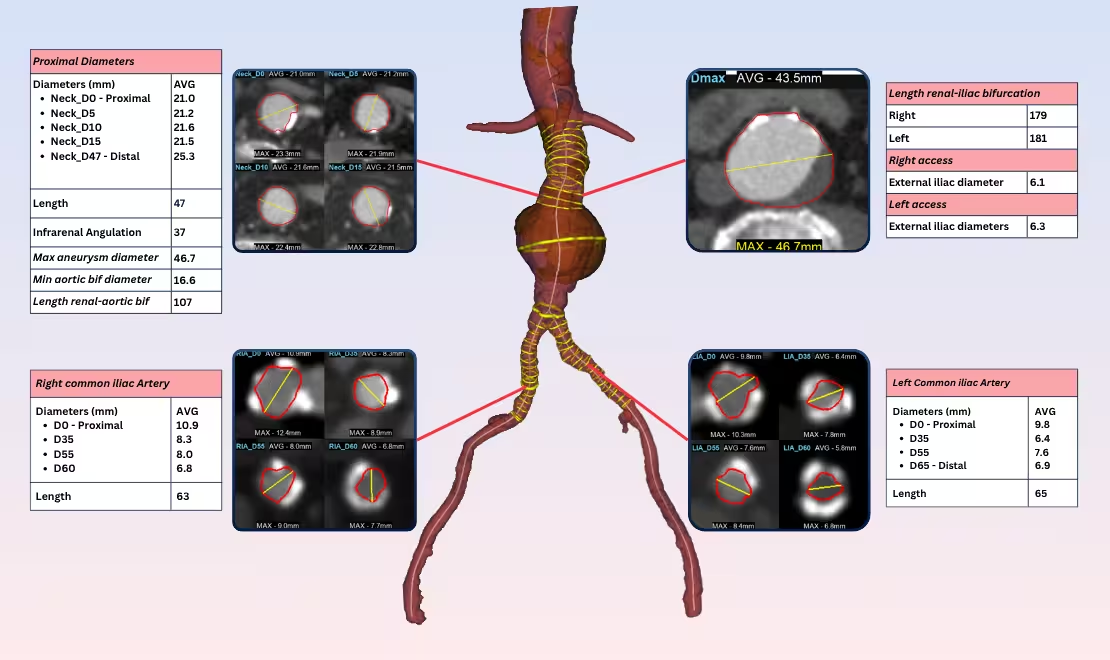
iSizing automates this entire process. After uploading the CT scan, iSizing performed automated segmentation of the aorta, identified thrombus and calcifications, and produced a comprehensive precise sizing report — all without manual measurement.
Every measurement was presented alongside cross-sectional CT views with automated vessel contours overlaid — giving Dr. Gallardo immediate visual confirmation of the iSizing work and the ability to interact with the 3D model to inspect any measurement in detail.
The entire sizing report was available for download with a single click in minutes automatically.
Why standardisation matters?
When the underlying measurements are standardised, the planning moves up a level. It is no longer "Do we trust these measurements?" It is "Which device best fits this anatomy?" That is where surgeon time and judgement actually generate value.
This is what standardisation gives: not just faster measurements, but measurements the surgeon can act on without second-guessing them.
EVAR Planning Agent — Choosing the optimal device
With the anatomy fully characterised, Dr. Gallardo moved to the planning phase directly within iSizing.
Rather than working from static measurements on paper, the platform allows surgeons to select a device from a built-in library and see it rendered in 3D on the patient's own anatomy in real time.
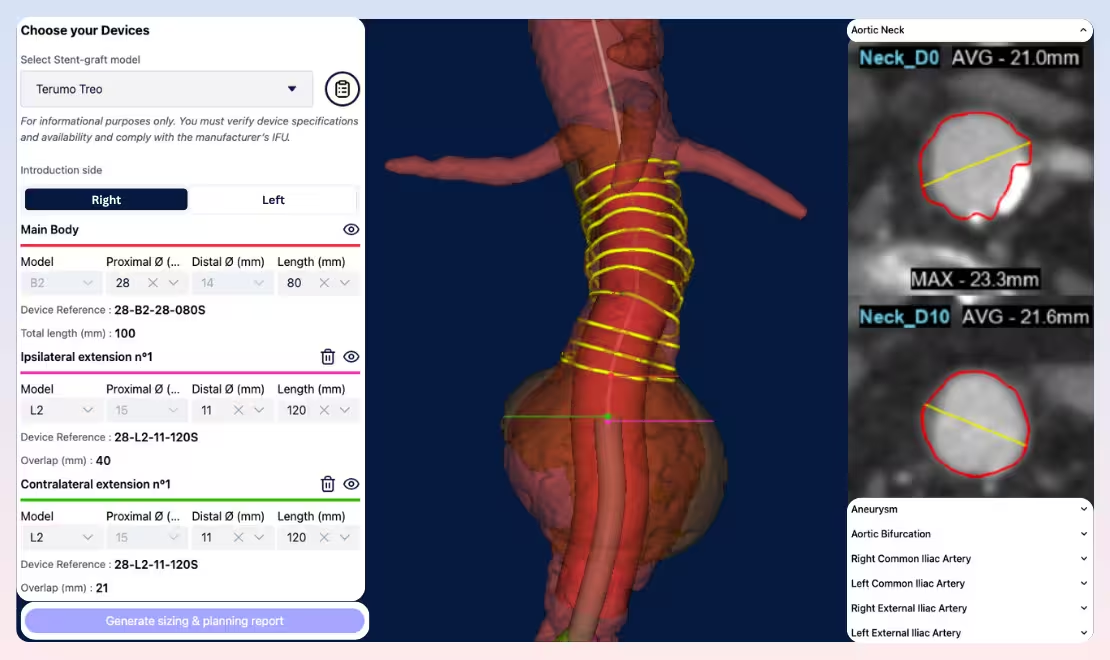
The interactive 3D model let Dr. Gallardo visualise how each component would sit relative to the aortic bifurcation and iliac vessels, adjust device selection as needed, and confirm adequate seal zones and overlap— all before the patient entered the operating room.
Once satisfied, iSizing generated a complete sizing and planning report in one click.
From plan to reality: The Intra-operative confirmation
The true test of any planning tool is how its projections hold up under fluoroscopy. In Dr. Gallardo's case, the intra-operative images confirmed what iSizing has given: Device positioning aligned with the pre-operative plan.
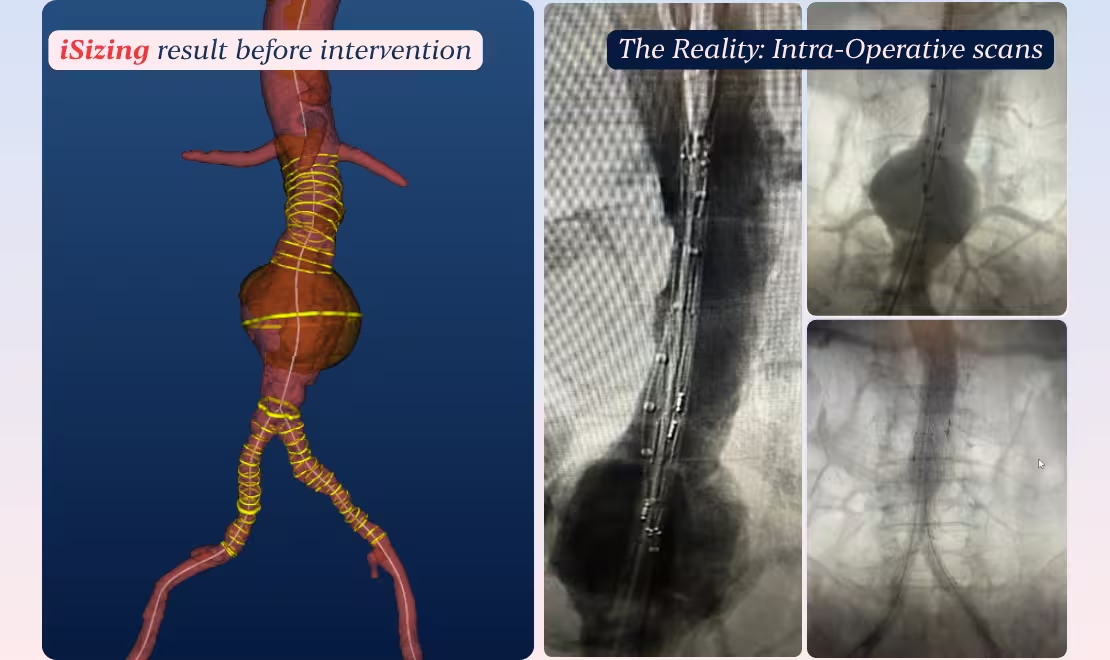
The correlation between the iSizing-generated plan and the intra-operative reality validated the accuracy of the automated measurements and the utility of the planning workflow — reducing uncertainty at every stage from CT review to device selection to deployment.
Conclusion
This case illustrates three core capabilities of iSizing:
- Speed without sacrifice: Automated segmentation and measurements deliver a complete sizing report in minutes, freeing vascular surgeons from manual measurement.
- Standardised measurements reducing variability: Instead of spending time arguing about the neck size either 21 mm or 22 mm, Vascular surgeons can spend it on whether the Treo 28 mm was the right oversize fort his specific neck behaviour, on which side to introduce, and on how to handle the iliac taper. That is where vascular surgeon`s judgement compounds.
- Integrated planning: Moving from measurements to device selection to visual confirmation in a single platform removes friction from the pre-operative workflow. Surgeons see the plan on the patient's actual anatomy, not an abstraction, before committing to a device order.
"The future of complex planning is not man versus machine, but expert clinicians empowered by intelligent tools."
— Dr. Fernando Gallardo, Head of Department, Angiology and Vascular Surgery, Hospital Quirónsalud, Marbella.