ERI in action: Assess the type 1A Endoleak Risk Index before the intervention.

Clinical Context
A challenging EVAR case is presented by Dr. Nilo J. Mosquera (Hospital Santiago de Compostela, Spain) involving a hostile proximal aortic neck—an anatomy known to increase the risk of Type IA endoleak. The standard pre-operative analysis alone was insufficient to confidently predict the outcome.
The key question was whether which size of the endograft would provide an adequate proximal seal and if the adjunction of endoanchors was necessary in this high-risk anatomy.
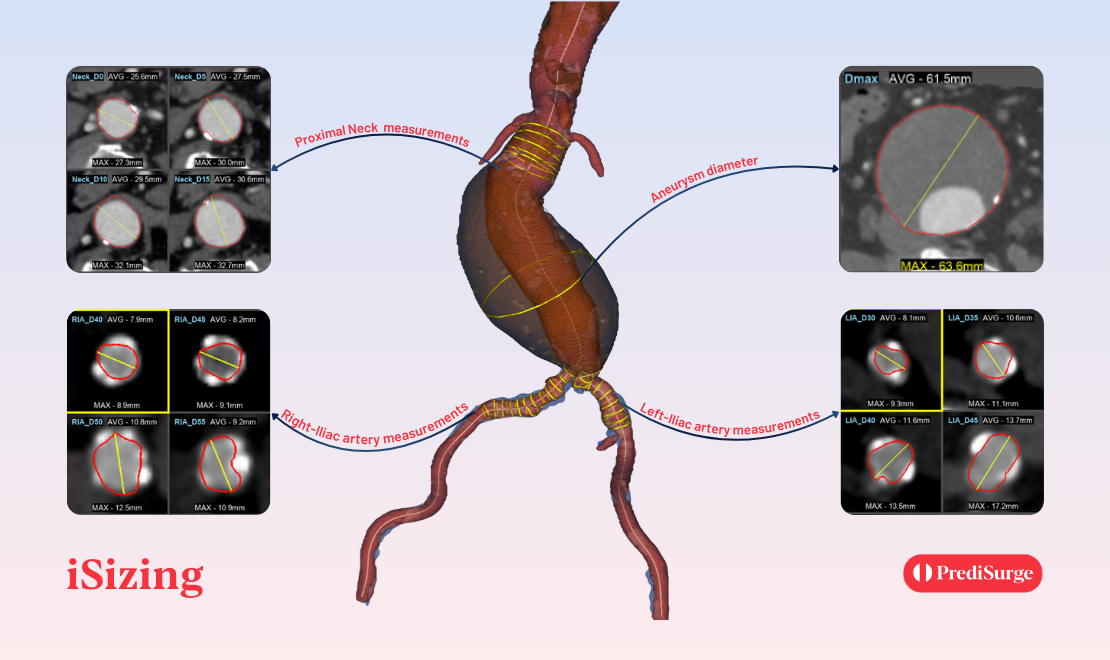
Case Overview: A Hostile Proximal Neck
The patient presented with a challenging proximal aortic neck characterized by multiple high‑risk features:
- Very short proximal neck (9 mm)
- Angulated and conical morphology
- Multiple risk factors for disease progression
- Absence of significant calcification
While the anatomy was clearly hostile, it remained within the instructions for use (IFU) for EndoSuture Aneurysm Repair (ESAR), keeping EVAR as a viable option. However, the key question remained: how high was the true risk of a Type IA endoleak, and how should it influence graft selection?
ERI Simulation: 32 mm vs 36 mm Endograft
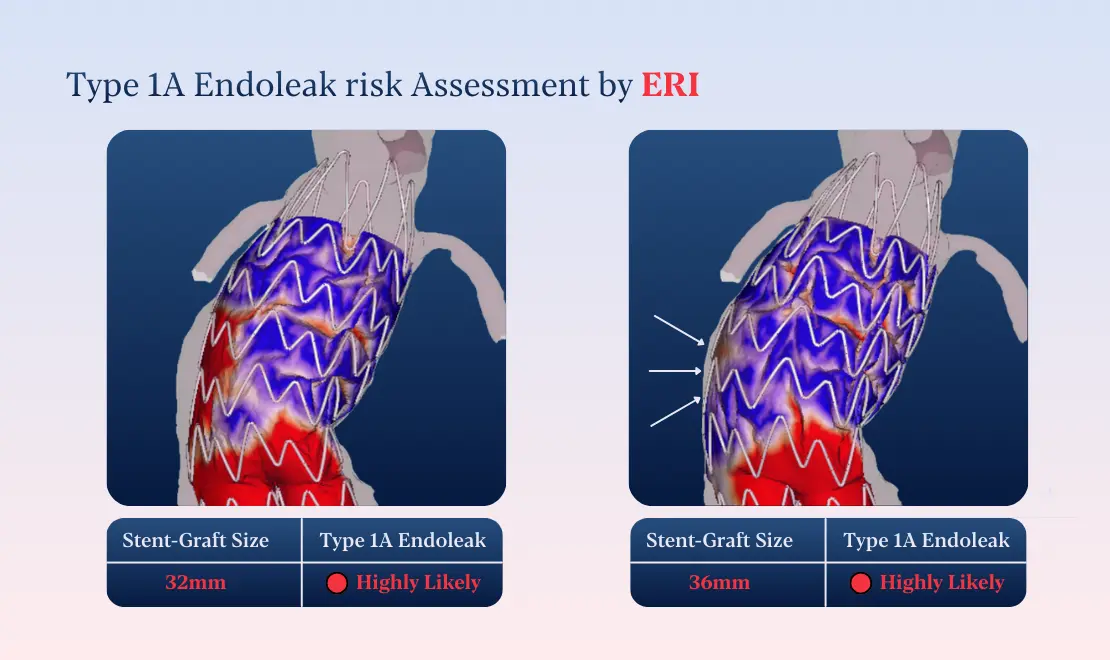
To support decision‑making, ERI simulations were performed comparing two potential main body sizes: 32 mm and 36 mm. The ERI analysis revealed a high likelihood of Type IA endoleak for both configurations.
These findings highlighted that oversizing alone would not mitigate risk in this anatomy and that the adjuction of endoanchors is necessary. Rather than replacing clinical judgment, ERI added a new layer of insight—quantifying risk before entering the operating room.
Intra-Operative Findings: ERI Predicts the Unseen
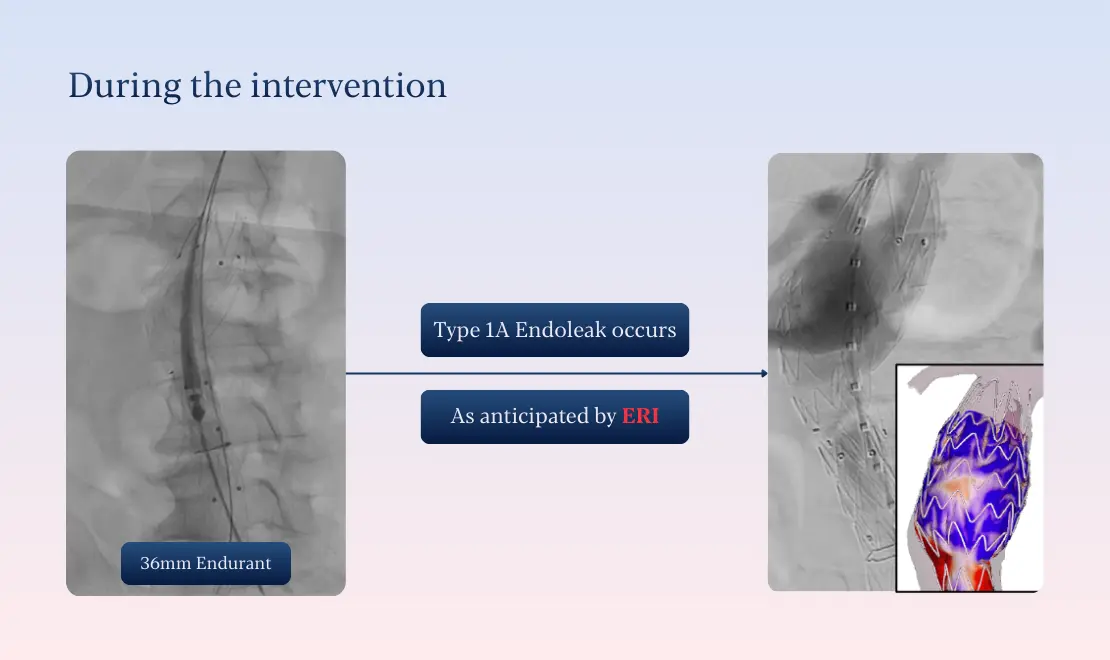
During the intervention, events unfolded exactly as anticipated. A Type IA endoleak occurred intraoperatively, confirming the ERI prediction. Rather than representing an unexpected complication, the endoleak was managed as a planned scenario.
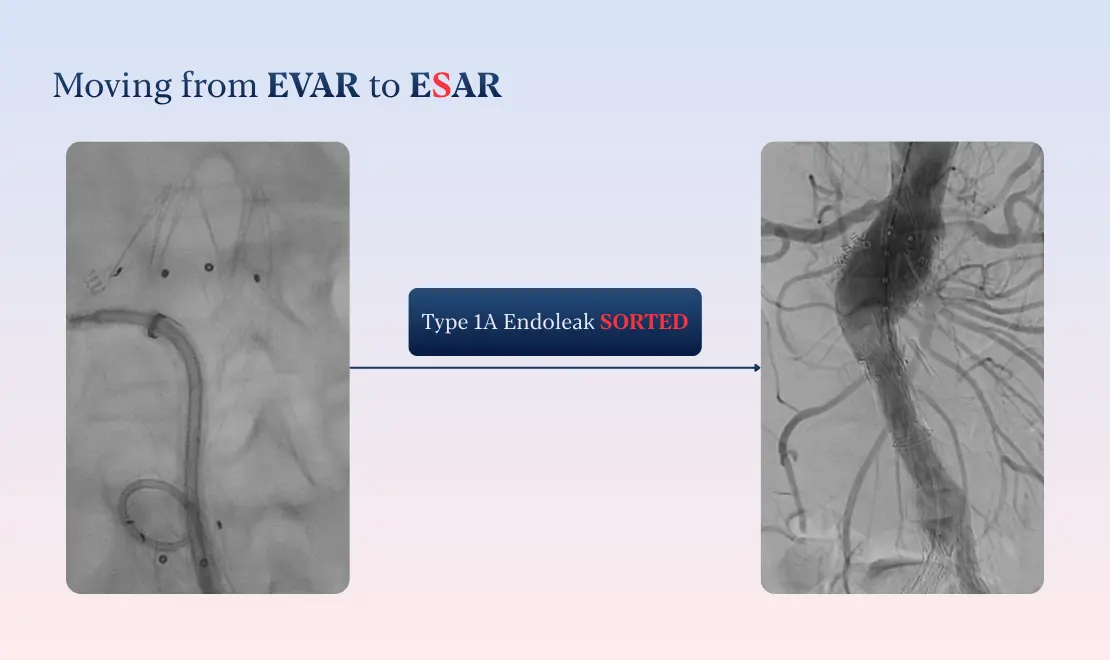
The surgical team promptly performed ESAR using EndoAnchors, successfully resolving the endoleak and stabilizing the proximal seal.
Outcome and Insight
This case clearly demonstrates the added value of ERI (Endoleak Risk Index) to your clinical practice:
- Optimized management of challenging or hostile anatomy
- Early assessment of peri-operative complication risks before the intervention
- Seamless comparison of clinical strategies to support the best treatment choice for each patient
Conclusion
ERI does not replace surgical expertise — it empowers it. By making the unseen visible, it supports vascular surgeons to move from reactive problem‑solving to proactive, precision‑guided intervention planning, aiming to better treat the challenging EVAR cases. As Dr. Nilo J. Mosquera commented: “AI models and digital twins can be a powerful tool for current practice. We need to take any advantage we can use to better treat our patients.”